



The findings presented below outline the outcomes of our literature search with respect to challenges, policies, and orphan drug regulations. Subsequently, a section dedicated to region-specific findings, derived from survey data and validation meetings is provided for each of the 5 domains.
Literature search
The sections below present the findings of our search into the challenges facing rare diseases and the policies implemented to mitigate them. Data were categorized into five domains: disease awareness, marketing authorization, reimbursement, pricing and HTA, orphan drug designation, and policy incentives and special access programs. Additionally, we provide an overview of orphan drug regulations in various countries.
Challenges & related policies
Disease awareness
There are several interrelated challenges associated with the recognition and diagnosis of rare diseases. Lack of awareness about a disease can impact both patients and physicians where patients who are unfamiliar with the specific signs and symptoms may not seek medical advice in a timely manner [20, 21]. Additionally, clinicians who lack awareness of rare diseases may be more likely to misdiagnose these conditions or delay making an accurate diagnosis [20, 21]. This is reflected in the significant delay in diagnosis experienced by many rare disease patients, with an average delay of 7.6 years in the United States and 5.6 years in the United Kingdom before getting the correct diagnosis [22]. On average, patients visit more than seven physicians before an accurate diagnosis is made [23].
Market authorization
Due to the rarity of such diseases, the available clinical evidence for these conditions is often limited. Therefore, decision-makers and regulators may be reluctant to grant approvals for rare disease treatments with such limited evidence [24]. In low and middle income countries, where awareness of rare diseases is even more limited, the approval process for these treatments can be slower than in higher income countries. Additionally, many Middle Eastern countries base their marketing authorization for rare disease treatments on approvals from the European Medicine Agency (EMA) and the FDA, which can further delay the initiation of the approval process and its regulation [1].
Policies to mitigate marketing authorization challenges of orphan drugs included the establishment of clear provisions and timelines for obtaining marketing authorization. For example, some countries provides fast-track approval for orphan drugs [6, 25].
Reimbursement, pricing, and HTA
The rarity of such diseases and difficulties facing pharmaceutical industries in developing their treatments drives industries to ask for high prices for their orphan drugs [26]. Some countries use external price referencing to determine the price of orphan drugs [27]. In response to that, pharmaceutical companies may employ a strategy known as “price sequencing,” which involves delaying the introduction of orphan drugs in lower economy markets to prevent other countries from referencing their lower prices which negatively affects patients access to treatment [27].
Regarding HTA, one major challenge for rare disease technologies is the absence of a tailored method for evaluating these technologies [28]. This can be attributed to several factors, including the lack of sufficient and robust clinical data [26], no established standard of care [29], insufficient knowledge of the natural history of these conditions, a lack of validated instruments for assessing efficacy and effectiveness endpoints, and the absence of an incremental cost-effectiveness threshold specifically designed for rare diseases [28, 30].
Another significant challenge is the uncertainty faced by HTA authorities when evaluating rare disease technologies. These technologies often have major uncertainties related to their real-world efficacy, effectiveness, cost-effectiveness, and added value [31]. Other uncertainties include the potential of the treatment to address unmet medical needs and the lack of strong evidence regarding the number of patients who may benefit from the treatment. This can result in uncertainty about the budget impact of these technologies, making it more difficult to inform decision-making and determine the value of orphan drugs [1, 24, 32].
To mitigate challenges related to the pricing and reimbursement of orphan drugs, pricing and reimbursement guidelines should be established. Furthermore, managed entry agreements and special access programs use should be increased to improve patient access to treatment [6]. Roessler et al. [33] reported methods that can be employed to control the high costs of orphan drugs such as the repurposing of drugs for new indications. However, this approach may be hampered due to financial considerations and difficulty in conducting clinical trials. Additionally, procurement mechanisms as price control, centralised purchasing and value-based procurement were utilized to reduce the economic impact of rare disease treatments. In an attempt to reduce the cost of the drug, partnerships and programs in collaboration with key stakeholders (such as the industry) may be established [34].
Since HTA is difficult to implement for orphan drugs due to very limited and non-robust data, Zelei et al. considered criteria to assess the value of orphan drugs. These criteria were classified into: disease-related criteria, treatment-related criteria, economic factors and societal factors [35]. These criteria can be translated into a tool to assess the value of orphan drugs.
Orphan drug designation
One of the challenges that faces rare disease and orphan drug designation is the lack of a universal accepted definition for rare diseases and orphan drugs [1]. The US FDA and the European Union (EU) define a drug intended to treat a rare disease as an orphan drug [5]. However, the threshold for what is considered a rare disease varies between regions.
Several policies were reported to regulate orphan drugs and mitigate such challenges. One of the policies included the establishment a formal definition and an official list for rare diseases [6]. The European Union (EU) defines rare diseases as life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people [36]. However, in the United States, the Food and Drug Administration (FDA) strictly defines rare diseases based only on their prevalence as any disease affecting fewer than 200,000 people [5].
Furthermore, establishing clear criteria for the drugs to be considered orphan (known as orphan designation) was stated in some countries [5, 6]. Criteria for granting orphan status to the drug mainly revolves around the intent of the drug to treat, prevent, diagnose a rare disease. For that reason, it is important to set a definition for rare disease.
Policy incentives & special access programs
Conducting research and clinical trials for rare diseases face several challenges, one of them is the limited number of patients and their dispersion across different geographic locations [37,38,39]. This makes it difficult to identify and recruit patients for clinical trials. Additionally, the limited number of rare disease experts and the heterogeneity of these conditions in terms of pathogenesis, symptom presentation, natural history, disease severity, and progression results in misdiagnosis and an underestimation of the true frequency of these diseases [1, 37, 40].
To address the challenges in research, several policies have been implemented to promote research and development. For instance, the EMA and FDA provide market exclusivity to orphan drugs for a period of 10 and 7 years, respectively [25, 41]. The EMA also offers assistance with clinical trial protocols and scientific advice to pharmaceutical companies developing orphan drugs [42]. In addition, some countries have established funding programs to support research and development in the field of rare diseases [6]. Research-related incentives also included protocol assistance, scientific advice, and clinical research subsidies [25].
There were also policy incentives related to increasing the market availability of orphan drugs. Payers can contribute to reducing the co-payment value incurred by patients. Furthermore, a funding program is also of great importance to increase access to orphan drugs. If the therapy is not provided in the country, then financial assistance for cross-border access may be beneficial. Tax credits for orphan drug sales are offered as an incentive for pharmaceutical industries. Furthermore, waiving fees or a fee refund for orphan drug submission files is also offered.
Special access programs play an increasingly important role in improving patient access to treatments for rare diseases. Several types of special access programs exist, each designed to increase patient access in different ways.
One type of special access programs is the early access program, which is implemented for patients after the discontinuation of a clinical trial. Under this type of program, the product is partially or fully funded from public funds, while the manufacturer gains additional data for marketing authorization purposes.
Another type of special access program is compassionate use, which allows an investigational product to be given to a group of patients who have a disease with no satisfactory authorized therapies and where there are no ongoing clinical trials [43].
Other types of special access programs include named patient basis early access, where the drug is designated for use by an individual patient, typically after the discontinuation of a clinical trial and before the drug is reimbursed [44].
In some cases, a product may be authorized for use in one indication but may also offer beneficial effects in another indication (off-label use). This is considered another form of special access programs [45].
Finally, coverage with evidence development is a form of special access programs, where payers agree to reimburse the drug, either as part of a clinical trial or through registered centres, while the manufacturer collects additional data [46].
Orphan drug regulations in different countries
In recent years, countries around the world started to pass laws and regulations aimed at improving patient access to orphan drugs. In the United States, for example, the Orphan Drug Act [47] provides incentives such as market exclusivity and tax credits to encourage the development of treatments for rare diseases [25]. Similarly, in Europe, incentives were provided, and in 2008, the European Union launched a project to facilitate the development of national plans for rare diseases [48]. In addition to these efforts, the European union launched a screening project with the goal of reducing the time required for diagnosis and enabling more efficient intervention through the use of genetic newborn screening and advanced analysis methods [49].
Non-EU countries also have national regulations to ensure coverage of orphan drugs. In Russia, for example, there is a special program that provides financing for 12 high-cost diseases at the federal level [50]. Countries like Australia, Japan, and Taiwan, offer incentives focusing on research and development where they provide financial and marketing incentives to develop and produce rare diseases medicines [25]. Incentives includes grants, fast-track approval, protocol assistance, and market exclusivity [50]. Similarly in Japan, it provides regulatory fee waivers, research grants, tax credits, and reductions, tools to reimburse medical costs, and funding to encourage research and orphan drug development [51, 52].
However, policies vary greatly between countries, for example, some countries in Latin America already have comprehensive rare disease policies such as the presence of healthcare plans with national centres and facilities to support disease management and guarantee access to health services. While other countries in Latin America, have only basic protective laws that do not necessarily guarantee funding or financial protection for patients, nor do they regulate access to treatments [25, 37, 47, 53, 54].
Rare diseases in the Middle East
The scientific literature describes numerous challenges related to managing rare diseases in the Middle East, especially a lack of access to genomic diagnostic tools and personalized care plans [55]. These challenges are exacerbated by the region’s high consanguinity rates and larger family sizes, which contribute to the elevated prevalence of rare conditions, especially Mendelian disorders [55]. Patients typically endure extended diagnostic journeys, averaging six to eight years, involving numerous hospital visits and redundant diagnostic tests [55]. This situation is further compounded by the shortage of skilled healthcare professionals, insufficient awareness of rare diseases, and inadequate reimbursement for genetic testing, resulting in delayed diagnosis and treatment and creating significant socio-economic burdens [19].
Efforts are underway to address these issues, such as the establishment of clinical genomic centers in some Middle Eastern countries, along with initiatives for genetic screening and counseling. For instance, a pilot project created the Catalogue of Transmission Genetics in Arabs (CTGA) database to improve education, raise public awareness, and track patients with rare diseases [19].
Collaborative efforts have also gained momentum, for instance, the UAE’s Rare Disease Society was formed to foster global scientific collaboration and promote awareness and prevention strategies [56]. Similarly, the Saudi Rare Disease Summit, held under the Saudi Ministry of Health, emphasizes multi-stakeholder collaboration to enhance patient care [57]. Additionally, the MENA Congress for Rare Diseases facilitates knowledge sharing and innovative strategies across the region, while the Centre for Arab Genomic Studies (CAGS) plays a pivotal role in characterizing genetic disorders and promoting research across Arab nations [58, 59].
In addition to the mentioned initiatives, Saudi Arabia has initiated programs to train nationals abroad to mitigate the shortage of skilled healthcare professionals in rare diseases [19].
There is a growing commitment to increasing the private sector’s role in healthcare. Pharmaceutical companies focus on marketing and distributing orphan drugs within the region.
On the policy front, the establishment of cost-effectiveness thresholds (CET) for orphan drugs in Egypt and the UAE have been introduced to prioritize and improve access to rare disease treatments. The Egyptian CET was established where the score of a Multi-Criteria Decision Analysis (MCDA) tool was translated into a multiplier of the conventional threshold to estimate a threshold for orphan drugs [60]. Additionally, the UAE has recently introduced its CET, incorporating a two-times multiplier specifically designed for treatments targeting rare diseases [61].
Local insights- survey and validation meetings
Disease awareness
Survey
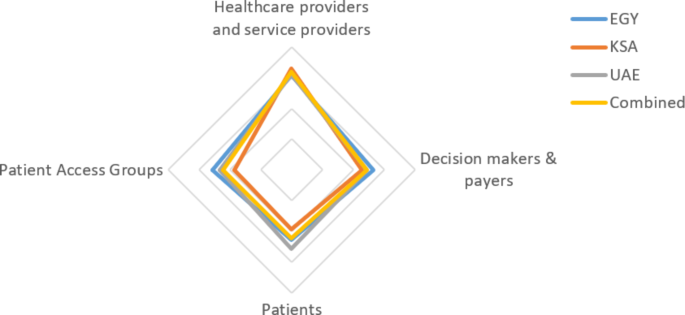
The first section of the survey was “disease awareness”. Respondents were asked to rate the level of awareness of different stakeholders on a scale from 1 (low) to 5 (high). The highest level of awareness for rare diseases in all countries was observed among healthcare and service providers. KSA had the highest level of awareness among healthcare providers, and the least among patients, and patient access groups for all countries combined. On the other hand, Egypt and UAE’s awareness levels were closely related as shown in Fig. 1.
Regarding national programs, almost 95% of respondents in all countries combined reported the absence of a national registry program. Additionally, more than 70% reported that there was no national screening program applied in their respective country or they weren’t aware of any. For diagnostic tools, most respondents (70%) in all countries combined indicated that diagnostic tools required were either lacking or not known to be readily available.

Validation meeting
Experts agreed with the survey results illustrating that the general level of awareness in all three countries is relatively low. They also stated that the highest level of awareness is observed among healthcare providers as they are in direct contact with patients. In Egypt, experts expected higher awareness among patients due to efforts by manufacturers to raise awareness.
In terms of national registries, KSA already deployed patient registries for some rare diseases. Egypt lacked a unified registry for rare disease patients and only has separate ones, such as the Health Insurance Organization’s (HIO) registry. While in UAE, experts stated that there are currently no known registries due to the lack of a surveillance system, but a new initiative using the International Classification of Diseases (ICD) codes 10 & 11 will be announced on the UAE national day.
Regarding the screening for rare diseases, experts in KSA indicated that newborn screening for hemophilia and spinal muscular atrophy is mandatory in both the public and private sectors. Experts in all countries reported that the availability of diagnostic tools varies as it is influenced by factors such as the existence of screening programs and availability of treatment. In UAE, if the required diagnostic tool is not available, the patient may be sent abroad for diagnosis.
Recommendations
Recommendations included the collaboration between the Ministry of Health (MoH) and pharmaceutical companies to improve rare disease policies, registries, awareness, and diagnosis. This can be achieved by increasing centers for diagnosis of rare diseases and training healthcare professionals on using diagnostic tools. In Egypt, it was recommended to develop a national plan aiming to mitigate rare diseases challenges. While in UAE, development of patient registries was recommended to decrease uncertainty in clinical evidence and improve patient access to drugs (Table 1).
Market authorization
Survey
More than half of the respondents reported that orphan drugs gain marketing authorization in a faster time compared to non-orphan drugs. Egypt was the slowest to acquire market authorization (12 months), while UAE was the fastest (6 months). The following figure shows the time needed by each country to grant orphan drug marketing authorization from the perspective of pharmaceutical companies (Fig. 2).
Concerning clinical evidence, more than half of pharmaceutical companies representatives in all countries reported that uncertainty in clinical evidence poses a hurdle in acquiring marketing authorization for rare diseases. Furthermore, more than 60% reported that regulatory bodies do not request local clinical evidence for orphan drugs.
As for the requirements of marketing authorization, more than 90% of respondents in all countries reported that FDA and/or EMA approvals were essential for orphan drugs to acquire marketing authorization locally. In KSA, approvals from the United Kingdom, Switzerland or Australia were considered in addition to the FDA or EMA. While in UAE, Japan approvals were considered on top of the FDA or EMA.
Validation meeting
In Egypt, experts reported that the marketing authorization process for orphan drugs takes either the same amount of time or even longer than non-orphan drugs. This is due to performing external price referencing (EPR) to set a price for orphan drugs. However, when EPR is not feasible, regulators may use value-based pricing, which takes even longer. In contrast, experts in UAE and KSA reported that marketing authorization for orphan drugs is faster than for non-orphan drugs.
In KSA, despite limited evidence for orphan drugs, they undergo a fast-track review and are authorized more quickly than non-orphan drugs. Egyptian experts reported the time required for marketing authorization to take is at least 18 months. While KSA experts reviewed 8.5 months reported by survey respondents as a reasonable duration, UAE experts indicated a maximum of 1 year for marketing authorization.
Experts in all countries agreed that uncertainty in clinical evidence poses a challenge in marketing authorization and an even greater issue in coverage and reimbursement of orphan drugs. According to experts, local evidence is not mandatory for market authorization in any of the three countries. However, experts in Egypt suggested that requesting local evidence could facilitate coverage and reimbursement decisions. For marketing authorization, all three countries mainly depend on submissions to the EMA or FDA.
Recommendations
Recommendations included the development of a separate registration process for orphan drugs with clearly identified requirements and timelines in all three countries (Table 1).
Reimbursement, pricing, and HTA
Survey
More than 80% of pharmaceutical companies representatives in the region reported the absence of provisions and guidelines for orphan drugs in both pricing and reimbursement. Regarding price referencing methodology for orphan drugs, all respondents agreed that external price referencing is applied to orphan drugs each in their respective country. Furthermore, 70% of respondents in the region mentioned that orphan drugs follow the regular process of formulary listing without any exemptions.
The shortest time needed for orphan drugs to be reimbursed was reported in the UAE with a median of 6 months while the longest time was reported in Egypt with a median of 18 months. In KSA, a median of 12 months was reported to reimburse orphan drugs.
Concerning the implementation of HTA for orphan drugs, half of the respondents in KSA reported that HTA is not used for orphan drugs. A similar percentage was reported in the UAE. However, in Egypt, more than 80% indicated that HTA is currently used for orphan drugs. Cost-effectiveness analysis was the most frequent component considered by respondents followed by budget impact analysis in all countries combined.
Regarding the cost-effectiveness threshold (CET), more than 70% in the region reported that CET is not applied for orphan drugs, or even if it is applied no special threshold is provided for orphan drugs.
Validation meeting
In Egypt, all respondents indicated that orphan drugs are priced according to EPR, but experts stated that when EPR is not feasible, value-based pricing may be used instead. In KSA, experts agreed with survey results that EPR is applied to orphan drugs. Experts also agreed with survey results that there are no pricing and reimbursement regulations for orphan drugs in the three countries. In terms of formulary listing, orphan drugs in Egypt follow the same process but are often rejected and fail to be listed. In that case, patients may access these drugs through media pressure or court orders. While, in KSA, orphan drugs can follow a different track depending on the authority listing them.
The time it takes for an orphan drug to be reimbursed after being authorized varies by country. In Egypt, experts considered 18 to 24 months a reasonable duration. In KSA, it may take less than 12 months to be reimbursed but longer to be listed. In UAE, experts agreed that it takes about 6 months for reimbursement, but timing also depends on the sector issuing the reimbursement decisions.
In Egypt, HTA is currently not used for assessing orphan drugs and UAE does not have an HTA process. Experts in all countries indicated that budget impact analysis is the most important criterion from the payer perspective. In Egypt, a differential threshold has been developed where multipliers of the cost-effectiveness threshold were used to determine the differential threshold for orphan drugs, but not yet implemented [60]. In the UAE, a recently established CET has been introduced, incorporating a differential threshold for rare diseases. For ultra-rare diseases, no threshold is required, and interventions are directly reimbursed for the individual [61]. In KSA, experts agreed on the importance of applying a higher value for orphan drugs when developing a threshold. Currently, the Saudi cost-effectiveness threshold has been published and is based on opportunity costs [62].
Recommendations
Recommendations for all three countries included establishing a pricing process for rare diseases that does not rely on external price referencing. It was also recommended to establish well-founded patient advocacy groups to allow for patient engagement in decision-making. In UAE and KSA, it was recommended to develop a cost-effectiveness threshold for non-orphan drugs and a higher differential cost-effectiveness threshold for orphan drugs. Furthermore, affordability programs to improve patient access to orphan drugs were also recommended. (Table 1)
Orphan drug designation
Survey
Most of the pharmaceutical companies representatives in the region responded that in their respective markets there are neither a definition nor a designation for rare diseases or orphan drugs. As for criteria required for orphan designation, nearly 90% of respondents indicated that there are no published criteria or procedures for orphan drug designation.
Validation meeting
Experts agreed with the survey results regarding the absence of an official definition and designation for rare disease or orphan drugs in their respective country. In KSA, experts stated that authorities follow the FDA definition for rare disease and orphan drugs.
Recommendations
Recommendations included the development of a guideline that considers how to identify rare diseases and implementing such guidelines in registration, pricing, and reimbursement. Since Egypt usually adopts the FDA or EMA for designation, it was recommended to formally announce it (Table 1).
Policy incentives & special access programs
Survey
Most of the policy incentives addressed in the survey were not applied in the region. Most respondents indicated that regulatory bodies neither grant market exclusivity for orphan drugs nor waive fees for orphan drug file submission each in their respective countries. A similar percentage of respondents reported that regulatory bodies do not provide tax credits or exemptions for orphan drug sales. Furthermore, almost all respondents indicated that orphan drugs follow regular price regulations with no exemptions. On the other hand, half the respondents supported the availability of funding programs for rare disease patients.
For special access programs implemented in the region, named patient basis early access was the most frequently implemented followed by compassionate use access schemes. While outcome-based managed entry agreements were known to be implemented by 50% of pharmaceutical companies’ representatives (Fig. 3).
Validation meeting
In terms of funding programs, experts in Egypt confirmed the existence of programs for rare diseases, such as the well-known initiative by the Egyptian president to provide free treatment for spinal muscular atrophy patients. In UAE and KSA, experts agreed with survey responses that there are no policy incentives in either country.
Regarding special access programs, experts in Egypt reported that there is currently no specific program for orphan drugs. Based on their experience, the most commonly implemented programs were patient early access and compassionate use. However, drugs are usually dispensed as a result a court order rather than a government decision.
Experts indicated that outcome-based agreements and coverage with evidence development are not implemented in Egypt. While in UAE, financial-based agreements are most commonly used. In KSA, early access programs are often used for rare diseases and outcome-based agreements are conducted for a small number of patients where a patient registry is formed, and physicians follow the patients while outcomes are collected by a third party.
Recommendations
Recommendations included increasing the use of MEAs and special access programs for orphan drugs in all countries. Since Egypt is a lower-middle income country, the use of outcome-based agreements to reduce the uncertainty in clinical evidence is recommended. Furthermore, combining outcome-based agreements with other agreements that mitigate the risk in the number of patients having the disease is suggested (Table 1).
Summary of recommendations for all domains (based on surveys and validation meetings)
A summary of proposed recommendations is summarized in Table 1.
link